
Choosing the Right Laser for Therapy: What Every Veterinarian Should Know
Laser therapy has become a widely accepted tool for treating a range of conditions in veterinary practice. While debates continue around which conditions it best addresses, one practical question remains highly relevant: What kind of laser should you be using?
Veterinarians today are faced with two primary options—Class 3b and Class 4 lasers. So, does the class really matter? The short answer is yes—but probably not in the way you think.
Understanding Laser Classes: It’s About Safety, Not Efficacy
Laser classifications are often misunderstood. These “classes” refer strictly to safety standards, not clinical performance.
- Class 3b lasers output up to 500 milliwatts (mW).
- Class 4 lasers output more than 500 mW.
The classification is based on the laser’s power and the potential risk to eyes or skin. For example, direct exposure to Class 3b light can damage your eyes, while even scattered light from a Class 4 laser can be hazardous without proper precautions. But again, this is about safety, not how well they work clinically.
best addresses, one practical question remains highly relevant: What kind of laser should you be using?
Veterinarians today are faced with two primary options—Class 3b and Class 4 lasers. So, does the class really matter? The short answer is yes—but probably not in the way you think.
The Origins of the Debate: Power vs. Caution
Historically, Class 3b lasers came first—not because they were the best, but because higher-powered systems simply didn’t exist. As Class 4 lasers emerged, a divide formed:
- Class 4 advocates promoted the “more power, better results” approach.
- Class 3b proponents warned about heat, safety, and “overexposure,” sometimes suggesting their lasers work via different mechanisms.
But do these claims hold up to scrutiny? Let’s look deeper.
Power Isn’t the Problem—It’s How You Use It
The effectiveness of laser therapy depends not just on power (Watts), but how that power is applied.
Imagine focusing a Class 3b beam into a pinpoint—you can burn the skin. Spread a Class 4 beam over a wider area, and the patient may not even feel it. The key parameter here is irradiance, or power per unit area. This determines whether your patient experiences warmth or discomfort—and it influences the clinical effect.
So what about the term “cold laser”?
Let’s be clear: there is no such thing as a cold laser in scientific terms. It’s a marketing term. All therapeutic lasers emit light, which is absorbed by the body and converted into heat within milliseconds. The difference in perceived heat comes down to how much light is delivered and over what area.
Want a Class 4 laser to feel “cold”? Just spread the beam or move it quickly. There’s no magic to it—only physics.
Overexposure Myths: A Matter of Dose, Not Danger
Another claim often made by Class 3b advocates is that Class 4 lasers risk “overexposing” tissue. But what does exposure really mean?
In laser therapy, exposure is the amount of energy delivered per unit area (called fluence, measured in Joules/cm²). It’s analogous to drug dosage—just as medication doses are based on body weight, laser therapy doses are based on surface area and time.
A Class 4 system can deliver the same dose as a Class 3b system, just faster. If used properly, overexposure is no more likely with a Class 4 laser than with a Class 3b. It’s a question of training and technique, not technology.
Depth Matters: Reaching the Target Tissues
Perhaps the most important clinical question is: Where do we want the laser energy to go?
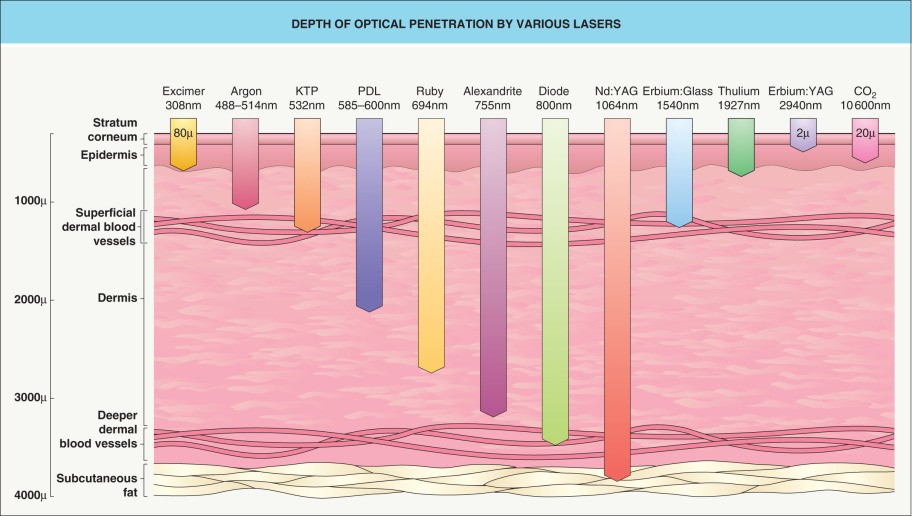
Laser light penetrates tissue, but its intensity decreases with depth. The rate of this decrease is described by penetration depth—the point where the energy has dropped to about 37% of its original intensity. Beyond that, light still travels deeper, but less of it gets through.
If your goal is to treat joints, tendons, or deep muscles, a low-power Class 3b laser may never deliver sufficient energy to those tissues. A Class 4 laser, however, can. The same therapeutic dose can be applied more deeply and effectively.
Skeptical? Consider this: if Class 3b lasers provide the ideal dose, at what depth is that dose achieved? The skin? The dermis? That may be fine for some applications—but not for conditions like osteoarthritis or deep-tissue injuries.
Not All Devices Are Created Equal
Let’s look at a real-world example. The Erchonia VLS laser emits just 7.5 mW per beam over a small area. That’s less than natural sunlight in the same spectrum. For context, the sun delivers about 6.5 mW/cm² in that wavelength range. Simply put: a walk in the sun may offer more light exposure than some Class 3b systems.
So, if you’re trying to treat a horse’s neck using such a device, you’d need weeks of continuous application to match the dose that a Class 4 system like the Eclipse®-VLS from OmniLase® can deliver in under 30 minutes.
The Bottom Line
There is nothing a Class 3b laser can do that a properly used Class 4 laser cannot—and often faster and more effectively. Concerns about “cold lasers,” “heat damage,” or “overexposure” are not rooted in physics or clinical science. They are artifacts of marketing and misunderstanding.
For veterinarians looking to deliver more efficient, targeted, and effective care, a Class 4 laser system offers superior flexibility and performance—with proper training and safety protocols, of course.
So next time you’re evaluating laser therapy systems, don’t just ask “Is this safe?” Ask “Can this actually reach the tissue I need to treat?”